Pain at the back of the heel or along the cord above it usually involves the Achilles tendon, the largest and strongest tendon in the body. Because the Achilles works with every step, irritation here tends to announce itself early in the morning, at the start of a run, or after a day with more walking than usual.
Achilles pain rarely appears out of nowhere. It usually reflects a change in load that the tendon was not prepared for. This article is general education for Beverly Hills and Los Angeles patients who are trying to understand the pattern and decide whether a podiatry visit makes sense.
How the Achilles tendon works
The Achilles tendon connects the calf muscles to the heel bone and transmits the force that pushes the body forward when walking, running, or climbing stairs. The loads passing through it are substantial, several times body weight during running, which is why the tendon is thick and strong. It is also why it is sensitive to sudden changes in demand. Tendon tissue adapts to load, but it adapts slowly, and pain often appears when activity increases faster than the tendon can keep up.
Common Achilles pain patterns
Clinicians generally describe two main locations of Achilles irritation. Midportion pain sits a few centimeters above the heel bone, along the cord itself, and is the most common overuse pattern, especially in runners and walkers. Insertional pain sits right where the tendon attaches to the back of the heel bone and is often aggravated by shoe pressure, uphill walking, and stretching into a deep ankle bend. A nearby fluid-filled cushion called a bursa can also become irritated and mimic tendon pain, and some people develop a bony prominence at the back of the heel that adds pressure under firm shoe counters.
Typical features across these patterns include stiffness with the first steps in the morning, pain at the start of activity that eases as the tendon warms up, tenderness when squeezing the tendon, and sometimes a thickened or swollen section of the cord.
Why overload happens
The triggers are usually ordinary changes rather than dramatic injuries:
- A sudden increase in walking, running mileage, or hill work.
- A switch to flatter or less supportive shoes without a transition period.
- New sports, new training surfaces, or a return to activity after time off.
- Long hours standing or walking at work.
- Tight or weak calf muscles that concentrate load on the tendon.
- Foot mechanics that change how the heel and tendon line up during gait.
Age plays a role as well, since tendon tissue tolerates rapid load changes less well over time. None of these factors mean activity is harmful. They mean the tendon responds best to gradual change.
Conservative care concepts
Most Achilles tendon irritation is managed without surgery. Patient-education sources such as Mayo Clinic and Cleveland Clinic describe a familiar set of conservative concepts: a temporary reduction in the activities that flare the pain, rather than complete rest; calf strengthening programs, which are a cornerstone of modern tendon care because tendons adapt to well-dosed load; a small heel lift or supportive footwear to reduce strain during daily walking; attention to shoe heel counters that press on a tender insertion; and a gradual, structured return to running or sport.
The right mix depends on whether the problem is midportion or insertional, how long it has been present, and what the person needs the tendon to do. That is why a focused exam is more useful than a generic protocol copied from the internet.
Warning signs that need prompt attention
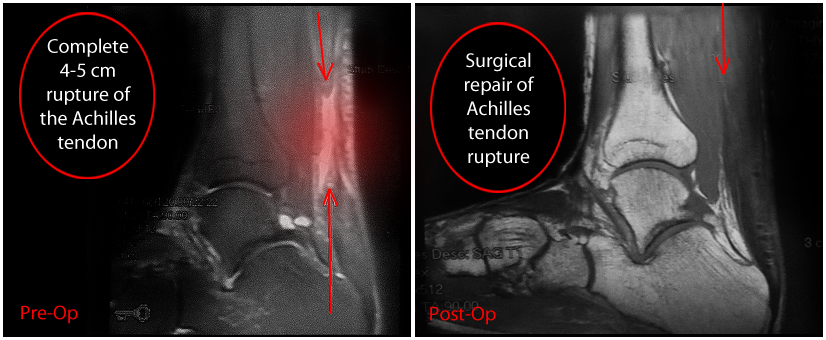
One scenario deserves urgent evaluation: a sudden snap or pop at the back of the ankle, often described as feeling like being kicked, followed by weakness pushing off, difficulty rising onto the toes, or a gap in the tendon. That pattern raises the question of an Achilles rupture, which is a different problem from gradual tendon irritation and is time-sensitive to evaluate.
Other findings that justify a prompt visit include pain that is severe or worsening rather than settling, significant swelling, redness and warmth over the tendon, pain following a direct injury, or symptoms in a person with diabetes or other conditions that affect healing.
When a podiatrist visit is reasonable
A podiatry visit makes sense when Achilles pain has lasted more than a couple of weeks, keeps returning each time activity resumes, limits walking or work, or is accompanied by any of the warning signs above. An exam can distinguish midportion tendon irritation, insertional problems, bursitis, and bony prominence pain, and can determine whether imaging would change the plan.
For patients in Beverly Hills and the greater Los Angeles area, the value of the visit is a plan matched to the actual diagnosis: the right loading program, the right footwear changes, and a realistic timeline. When conservative care has been given a fair trial and the tendon still will not settle, a podiatrist can also walk through the next-level options and what each one involves.
General next steps
Achilles pain that follows a recent change in activity often improves with load management, calf strengthening, and footwear adjustments applied patiently over weeks. Sudden pops, push-off weakness, or pain that persists despite sensible care are reasons to seek evaluation promptly rather than continuing to push through it.
Medical disclaimer: This article is general information about Achilles tendon pain. It is not medical advice, a diagnosis, or a treatment recommendation. Foot and ankle care depends on your symptoms, exam findings, medical history, and goals. Consult a licensed podiatrist or qualified healthcare professional for evaluation of your specific situation.